
 Dermatoscope and Magnifiers
Dermatoscope and Magnifiers Diagnostic Kits
Diagnostic Kits Vital Signs Monitors
Vital Signs Monitors Stethoscopes and Accessories
Stethoscopes and Accessories Otoscopes, Ophthalmoscopes, and Retinoscopes
Otoscopes, Ophthalmoscopes, and Retinoscopes Reflex Hammers and Neurological Tools
Reflex Hammers and Neurological Tools Scales and Measuring Devices
Scales and Measuring Devices Spirometers and Pulmonary Function Tests
Spirometers and Pulmonary Function Tests
 Electrosurgical Units and Accessories
Electrosurgical Units and Accessories Cutting Instruments
Cutting Instruments Grasping and Holding Instruments
Grasping and Holding Instruments Hemostatic Instruments
Hemostatic Instruments Specialized Surgical Sets
Specialized Surgical Sets Single-Use Procedure Trays and Packs
Single-Use Procedure Trays and Packs Surgical Drapes, Gowns, and Covers
Surgical Drapes, Gowns, and Covers Tissue Unifying Instruments
Tissue Unifying Instruments
 Radiation Protection
Radiation Protection X-Ray Machines and Accessories
X-Ray Machines and Accessories Ultrasound Systems and Probes
Ultrasound Systems and Probes MRI and CT Scanners
MRI and CT Scanners Radiology Consumables
Radiology Consumables Bone Densitometers
Bone Densitometers Fluoroscopy Equipment
Fluoroscopy Equipment Imaging Tables and Positioning Aids
Imaging Tables and Positioning Aids
 Microscopes and Accessories
Microscopes and Accessories Centrifuges and Separators
Centrifuges and Separators Analyzers
Analyzers Incubators and Ovens
Incubators and Ovens Pipettes, Dispensers, and Lab Glassware
Pipettes, Dispensers, and Lab Glassware Refrigerators, Freezers, and Storage Units
Refrigerators, Freezers, and Storage Units Lab Consumables
Lab Consumables Sterilizers and Autoclaves for Lab Use
Sterilizers and Autoclaves for Lab Use
 Multi-Parameter Monitors
Multi-Parameter Monitors Ventilators and Respiratory Support Devices
Ventilators and Respiratory Support Devices Defibrillators and AEDs
Defibrillators and AEDs Infusion Pumps and IV Systems
Infusion Pumps and IV Systems Patient Warmers and Cooling Devices
Patient Warmers and Cooling Devices Central Monitoring Stations
Central Monitoring Stations Accessories
Accessories
 Anesthesia Machines and Workstations
Anesthesia Machines and Workstations Oxygen Concentrators and Delivery Systems
Oxygen Concentrators and Delivery Systems Nebulizers and Inhalers
Nebulizers and Inhalers CPAP/BiPAP Machines
CPAP/BiPAP Machines Airway Management
Airway Management Anesthesia Masks, Circuits, and Bags
Anesthesia Masks, Circuits, and Bags Humidifiers and Heaters
Humidifiers and Heaters Respiratory Therapy Accessories
Respiratory Therapy Accessories
 First Aid Kits and Cabinets
First Aid Kits and Cabinets Emergency Resuscitation Equipment
Emergency Resuscitation Equipment Trauma Supplies
Trauma Supplies Emergency Carts and Crash Carts
Emergency Carts and Crash Carts Burn Care Products
Burn Care Products Bleeding Control
Bleeding Control Automated External Defibrillators (AEDs)
Automated External Defibrillators (AEDs) Transport and Evacuation
Transport and Evacuation
 Wheelchairs and Accessories
Wheelchairs and Accessories Walkers, Crutches, and Canes
Walkers, Crutches, and Canes Prosthetics and Orthotics
Prosthetics and Orthotics Physical Therapy Equipment
Physical Therapy Equipment Transfer Devices
Transfer Devices Bathroom Safety
Bathroom Safety Orthopedic Traction and Tables
Orthopedic Traction and Tables Hot/Cold Therapy Packs and Units
Hot/Cold Therapy Packs and Units
 Beds and Mattresses
Beds and Mattresses Chairs and Stools
Chairs and Stools Tables
Tables Cabinets and Storage
Cabinets and Storage Privacy Screens & Curtains
Privacy Screens & Curtains Stands and Racks
Stands and Racks Linens and Textiles
Linens and Textiles Lighting
Lighting
 Autoclaves and Sterilizers
Autoclaves and Sterilizers Ultrasonic Cleaners
Ultrasonic Cleaners Disinfectant Solutions and Wipes
Disinfectant Solutions and Wipes Sterilization Pouches, Wraps, and Indicators
Sterilization Pouches, Wraps, and Indicators Instrument Trays and Containers
Instrument Trays and Containers UV and Ozone Disinfection Devices
UV and Ozone Disinfection Devices Washer Disinfectors
Washer Disinfectors
 Wound Care
Wound Care Gloves
Gloves Masks and Respirators
Masks and Respirators Catheters and Tubing
Catheters and Tubing Swabs, Applicators, and Sponges
Swabs, Applicators, and Sponges Incontinence Products
Incontinence Products Personal Protective Equipment (PPE)
Personal Protective Equipment (PPE)
 Dental Chairs and Units
Dental Chairs and Units Handpieces and Burs
Handpieces and Burs Instruments
Instruments Consumables
Consumables Sterilization for Dental Use
Sterilization for Dental Use Orthodontic Supplies
Orthodontic Supplies Endodontic Tools
Endodontic Tools
 Slit Lamps and Tonometers
Slit Lamps and Tonometers Lensometers and Phoropters
Lensometers and Phoropters Ophthalmic Surgical Instruments
Ophthalmic Surgical Instruments Eyewear Frames and Lenses
Eyewear Frames and Lenses Contact Lens Supplies
Contact Lens Supplies Vision Testing Charts and Devices
Vision Testing Charts and Devices Eye Care Consumables
Eye Care Consumables Laser Systems for Eye Care
Laser Systems for Eye Care
 ENT Exam Chairs and Tables
ENT Exam Chairs and Tables Endoscopes
Endoscopes Audiometers and Hearing Tests
Audiometers and Hearing Tests ENT Instruments
ENT Instruments Nasal and Throat Packs
Nasal and Throat Packs Hearing Aids and Accessories
Hearing Aids and Accessories Otology Supplies
Otology Supplies
 Fetal Dopplers and Monitors
Fetal Dopplers and Monitors Delivery Beds and Tables
Delivery Beds and Tables Gynecological Instruments
Gynecological Instruments Neonatal Incubators and Warmers
Neonatal Incubators and Warmers Breast Pumps and Accessories
Breast Pumps and Accessories Contraceptive Devices
Contraceptive Devices Maternity Supports and Pads
Maternity Supports and Pads Neonatal Consumables
Neonatal Consumables
 Cystoscopes and Urethroscopes
Cystoscopes and Urethroscopes Dialysis Machines and Supplies
Dialysis Machines and Supplies Urological Catheters and Bags
Urological Catheters and Bags Lithotripters
Lithotripters Prostate Treatment Devices
Prostate Treatment Devices Urinary Incontinence Products
Urinary Incontinence Products Kidney Stone Management Tools
Kidney Stone Management Tools Consumables & Disposables
Consumables & Disposables
 EEG and EMG Machines
EEG and EMG Machines Neurosurgical Instruments
Neurosurgical Instruments Nerve Stimulators
Nerve Stimulators Headrests and Positioning Aids
Headrests and Positioning Aids Lumbar Puncture Kits
Lumbar Puncture Kits Seizure Monitoring Devices
Seizure Monitoring Devices Consumables
Consumables Rehabilitation for Neurological Conditions
Rehabilitation for Neurological Conditions
 ECG Machines and Accessories
ECG Machines and Accessories Holter Monitors
Holter Monitors Stress Test Systems
Stress Test Systems Pacemakers and Defibrillator Accessories
Pacemakers and Defibrillator Accessories Vascular Access Devices
Vascular Access Devices Cardiac Catheters and Guidewires
Cardiac Catheters and Guidewires Blood Flow Meters
Blood Flow Meters Consumables
Consumables
 Orthopedic Instruments
Orthopedic Instruments Casts, Splints, and Padding
Casts, Splints, and Padding Joint Replacement Supplies
Joint Replacement Supplies Prosthetic Limbs and Components
Prosthetic Limbs and Components Bone Grafts and Substitutes
Bone Grafts and Substitutes Traction Devices
Traction Devices Orthopedic Braces and Supports
Orthopedic Braces and Supports Rehabilitation Aids for Orthopedics
Rehabilitation Aids for Orthopedics
 Home Oxygen Therapy
Home Oxygen Therapy Hospital Beds for Home Use
Hospital Beds for Home Use Mobility Aids
Mobility Aids Bathroom and Daily Living Aids
Bathroom and Daily Living Aids Wound Care for Home
Wound Care for Home Monitoring Devices
Monitoring Devices Enteral Feeding Pumps and Tubes
Enteral Feeding Pumps and Tubes
 Hand Sanitizers and Dispensers
Hand Sanitizers and Dispensers Face Shields and Goggles
Face Shields and Goggles Isolation Gowns and Suits
Isolation Gowns and Suits Biohazard Waste Containers
Biohazard Waste Containers Air Purifiers and HEPA Filters
Air Purifiers and HEPA Filters Surface Disinfectants
Surface Disinfectants Sharps Containers
Sharps Containers Protective Barriers
Protective Barriers
 Cardiovascular & Endurance Training
Cardiovascular & Endurance Training Strength Training & Weightlifting
Strength Training & Weightlifting Functional Training & Core Conditioning
Functional Training & Core Conditioning Physical Therapy & Rehabilitation
Physical Therapy & Rehabilitation Sports & Outdoor Recreation
Sports & Outdoor Recreation Gym Flooring & Facility Equipment
Gym Flooring & Facility Equipment Fitness Monitoring & Accessories
Fitness Monitoring & Accessories Kids & Novelties
Kids & Novelties















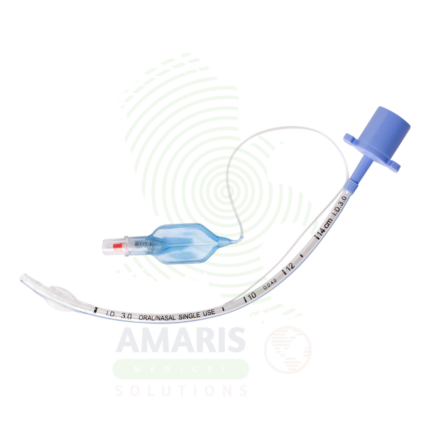
Cuffed Endotracheal Tubes
Cuffed Endotracheal Tubes are flexible airway devices with an inflatable cuff designed for secure airway management during positive pressure ventilation and aspiration prevention. The high-volume, low-pressure cuff creates a seal within the trachea, preventing air leakage and aspiration of gastric contents. Essential for anesthesia, intensive care, and emergency medicine, they provide reliable airway protection for patients requiring mechanical ventilation.

Endotracheal Tube Introducer ( Bougie)
An Endotracheal Tube Introducer (Bougie) is a semi-rigid, flexible guide used to facilitate endotracheal intubation in difficult airway scenarios. Providing tactile feedback through characteristic clicks as it passes over tracheal rings, it serves as a rescue device when direct laryngoscopy fails. Essential for anesthesia, emergency medicine, and critical care, it is a standard component of difficult airway management algorithms.

Flexible Fiber Optic Laryngoscope
A Flexible Fiber Optic Laryngoscope is a flexible endoscope (2-5 mm diameter, 30-60 cm working length) with fiber optic image transmission and steerable tip (120-180° angulation) for visualization of the upper airway and facilitation of difficult intubations. Features include control handle with angulation lever, working channel (1-2 mm) for suction or oxygen, external light source (halogen/xenon/LED), and optional camera for video display. Primary clinical applications include awake intubation in difficult airway management (limited mouth opening, cervical spine instability, obstructing pathology), nasotracheal intubation for oral surgery or maxillofacial trauma, intubation with cervical spine precautions (minimal neck movement), diagnostic airway assessment (stridor, hoarseness, vocal cord dysfunction, masses), double-lumen tube placement for thoracic surgery, pediatric difficult airway management, and tracheostomy tube placement guidance. Class II medical device requiring FDA clearance. Critical safety considerations include mandatory leak testing before immersion, antifog preparation, gentle insertion technique, airway maintenance with oxygen, topical anesthesia for patient comfort, suction availability, backup airway device, and strict infection control with validated reprocessing protocols.

Intubating Stylet
An Intubating Stylet is a malleable or pre-shaped semi-rigid rod inserted into an endotracheal tube to provide shape, rigidity, and directional control for tracheal intubation, particularly in difficult airway management. The malleable metal core allows the clinician to bend the stylet-tube assembly into customized shapes (hockey stick, J-shape, or patient-specific curve) to navigate anatomical variations such as anterior larynx, large tongue, cervical spine immobility, or congenital abnormalities. For the anesthesiologist, intensivist, and emergency physician, the intubating stylet increases first-pass intubation success, reducing the risk of hypoxia, aspiration, and airway-related complications during emergency or surgical airway management. The smooth polymer coating reduces friction, while the atraumatic tip minimizes the risk of airway trauma during insertion. Available in various lengths (adult, pediatric, nasal) and diameters (5Fr to 15Fr) for different endotracheal tube sizes, with both single-use disposable and reusable sterilizable options, the intubating stylet is an essential component of difficult airway carts and standard airway management protocols.

Macintosh Bulb Laryngoscope
A Macintosh Bulb Laryngoscope is a rigid laryngoscope with curved Macintosh blade (sizes 0-4, 70-160 mm) featuring a distal incandescent (xenon, krypton, halogen) or LED bulb at the blade tip for direct illumination during tracheal intubation. The curved blade design allows indirect epiglottis elevation by placing the tip in the vallecula, requiring less force and neck extension than straight blades. Features stainless steel reusable blades (or disposable plastic), ergonomic handles with knurled grip, ISO standard hook-on fittings, and autoclavable options. Light output 500-3,000 Lux depending on bulb type and battery condition. Primary clinical applications include routine and emergency tracheal intubation during general anesthesia, difficult airway management, cervical spine precautions (minimal neck movement), rapid sequence intubation, neonatal and pediatric intubation (sizes 0-2), teaching and training, and use in resource-limited settings. Class II medical device requiring FDA clearance. Critical safety considerations include pre-use light check (brightness, bulb security), appropriate blade size selection, proper lifting technique (not levering on teeth), battery verification, bulb obstruction risk from secretions, backup device availability, and infection control (sterilization or disposable blades).

Macintosh Fiber Optic Laryngoscope
A Macintosh Fiber Optic Laryngoscope is a rigid laryngoscope with curved Macintosh blade (sizes 0-4, 70-160 mm) incorporating an integrated fiber optic light bundle that transmits bright, focused illumination (2,000-10,000+ Lux) from a handle-mounted LED or xenon bulb to the blade tip for enhanced visualization during tracheal intubation. The curved blade design allows indirect epiglottis elevation by placing the tip in the vallecula, requiring less force and neck extension than straight blades. Features stainless steel reusable blades, ergonomic handles with knurled grip, ISO standard hook-on fittings, and steam autoclave compatibility. Primary clinical applications include routine and emergency tracheal intubation during general anesthesia, difficult airway management with improved illumination, cervical spine precautions (minimal neck movement), teaching and training (enhanced visualization for instructors), rapid sequence intubation, neonatal and pediatric intubation (sizes 0-2), and oral/maxillofacial surgery. Class II medical device requiring FDA clearance. Critical safety considerations include pre-use light check (dark spots indicate broken fibers), appropriate blade size selection, proper lifting technique (not levering on teeth), battery verification, fiber optic care (avoid sharp bending), and backup device availability.

Miller Bulb Laryngoscope
A Miller Bulb Laryngoscope is a rigid laryngoscope with straight Miller blade (sizes 0-4, 70-160 mm) featuring a distal incandescent (xenon, krypton, halogen) or LED bulb at the blade tip for direct illumination during tracheal intubation. The straight blade design allows direct elevation of the epiglottis rather than the indirect vallecula technique, making it the preferred choice for pediatric and neonatal intubation, patients with floppy or prominent epiglottis, and anterior airways requiring direct epiglottic control. Features stainless steel reusable blades (or disposable plastic), ergonomic handles with knurled grip, ISO standard hook-on fittings, and autoclavable options. Light output 500-3,000 Lux depending on bulb type and battery condition. Primary clinical applications include direct epiglottis elevation for tracheal intubation (especially pediatric and neonatal), patients with prominent or floppy epiglottis, anterior airway management, teaching and training (straight blade technique), neonatal resuscitation, and use in resource-limited settings. Class II medical device requiring FDA clearance. Critical safety considerations include pre-use light check (brightness, bulb security), appropriate blade size selection (especially critical in pediatrics), proper lifting technique (direct epiglottic lift, not levering on teeth), pediatric fragility awareness, bulb obstruction risk from secretions, battery verification, and backup device availability.

Miller Fiber Optic Laryngoscope
A Miller Fiber Optic Laryngoscope is a rigid laryngoscope with straight Miller blade (sizes 0-4, 70-160 mm) incorporating an integrated fiber optic light bundle that transmits bright, focused illumination (2,000-10,000+ Lux) from a handle-mounted LED or xenon bulb to the blade tip for enhanced visualization during tracheal intubation. The straight blade design allows direct elevation of the epiglottis rather than the indirect vallecula technique, making it particularly useful for pediatric/neonatal intubation, patients with floppy or prominent epiglottis, anterior airways, and difficult airways requiring direct epiglottic control. Features stainless steel reusable blades, ergonomic handles with knurled grip, ISO standard hook-on fittings, and steam autoclave compatibility. Primary clinical applications include direct epiglottis elevation for tracheal intubation (especially pediatric and neonatal), difficult airway management with fiber optic illumination, patients with prominent or floppy epiglottis, cervical spine precautions, anterior airway management, teaching and training (straight blade technique), and neonatal resuscitation. Class II medical device requiring FDA clearance. Critical safety considerations include pre-use light check (dark spots indicate broken fibers), appropriate blade size selection (especially critical in pediatrics), proper lifting technique (direct epiglottic lift, not levering on teeth), pediatric fragility awareness, battery verification, fiber optic care (avoid sharp bending), and backup device availability.

Suction Catheters
Suction Catheters are sterile, single-use flexible tubes designed for aspiration of pulmonary secretions from the airways of intubated, tracheostomized, or spontaneously breathing patients unable to clear their own secretions. Available in French sizes 5 Fr-18 Fr, with whistle-tip or coude configurations, single or multiple eyelets, and thumb-controlled suction valves. Open suction catheters are single-pass devices requiring strict sterile technique and immediate disposal. Closed (in-line) suction catheters are enclosed in a sterile sheath, permitting suctioning without ventilator disconnection, maintaining PEEP, and reducing aerosolization of pathogens—essential for high-frequency ventilation, ARDS, and airborne precautions. Critical safety parameters include catheter gauge not exceeding one-half the endotracheal tube internal diameter, suction duration ≤15 seconds, and vacuum pressure ≤150 mmHg. Proper technique prevents hypoxemia, mucosal trauma, and ventilator-associated pneumonia.

Tracheostomy Tube
A Tracheostomy Tube is a curved, sterile medical device inserted through a surgical opening in the trachea to establish and maintain a secure airway for patients requiring long-term mechanical ventilation, upper airway obstruction management, or effective secretion clearance. Constructed from medical-grade PVC, silicone, or polyurethane, these tubes feature an outer cannula, removable inner cannula for patency maintenance, and a high-volume, low-pressure cuff to prevent aspiration and enable positive pressure ventilation. Available in pediatric through adult sizes with fenestrated options for speech, tracheostomy tubes are essential devices in intensive care units, long-term care facilities, and home care settings. For the clinician, they provide stable airway access that facilitates mechanical ventilation, weaning, and rehabilitation. For the patient, a tracheostomy tube enables improved comfort, mobility, communication, and quality of life compared to prolonged endotracheal intubation.
Uncuffed Endotracheal Tubes
Uncuffed Endotracheal Tubes are flexible airway devices designed for pediatric and neonatal patients, short-term ventilation, and nasotracheal intubation. The absence of an inflatable cuff reduces the risk of tracheal injury in developing airways while providing adequate ventilation. Used in pediatric anesthesia, neonatology, and emergency medicine, they are essential for safe airway management in patients where cuffed tubes may pose increased risk.








